
Keywords
transhiatal esophagectomy
transthoracic esophagectomy
Abstract
Introduction: The authors present the results of surgical treatment of esophageal cancer at Department of Surgery I, University Hospital Olomouc between 2006−2016. The aim of the study was to use retrospective analysis to evaluate the results of patients operated for esophageal cancer and statistically evaluate the results based on the type of surgical approach (transhiatal, transthoracic).
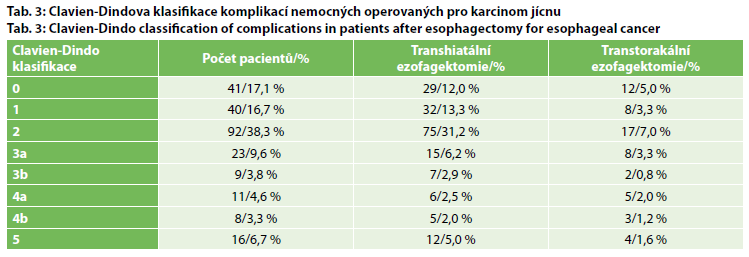
Method: A total of 240 patients with esophageal cancer were operated at Department of Surgery I between the beginning of 2006 and the end of 2016. We evaluated respiratory complications, the incidence of anastomotic fistula and complications based on the Clavien-Dindo classification of complications, based on the type of surgical approach selected (transhiatal or transthoracic esophagectomy).
Results: The patient set included 207 men (86.3%) and 33 women (13.7%). The mean patient age was 60.4 years. The histological type was adenocarcinoma in 145 (60.4%) and squamous cell carcinoma in 90 (37.5%) patients; another type of carcinoma was observed in 5 cases. Transhiatal esophagectomy was performed in 194 patients (80.2%) (transhiatal laparoscopic in 190 and classic Orringer in 4 patients). Transthoracic approach was used in 46 patients (19.2%), thoracoscopic in 16, and thoracotomic in 30 patients. A gastric conduit was used in 236 patients and coloplasty was performed in 4 patients. The mean duration of surgery was 217 min for the transhiatal approach, 239 min for the thoracoscopic approach and 277 min for the thoracotomic approach. Total blood loss per patient was 562 ml on average for all the operated patients. Peri- or postoperative blood transfusions were administered to 148 patients. Lymphadenectomy was performed as part of the procedure in all patients; the mean of 16.1 lymph nodes were removed. The average hospital stay was 20.7 days. In the patient set, 30-day mortality included 12 patients (respiratory complications 10, MI 1, conduit necrosis 1) and 90-day mortality included 4 (multi organ failure during ARDS). Based on statistical analysis, the incidence of respiratory complications significantly correlated with ASA classification (p=0.0001) and Clavien-Dindo classification (p<0.0001). ASA score 3 was significantly more common and ASA score 2 uncommon in patients with severe respiratory complications (respiratory failure, ARDS) compared to patients without respiratory complications. Furthermore, patients with severe complications were significantly more commonly classified as Clavien-Dindo 4 and 5 compared to patients with less severe or no respiratory complications. Based on statistical analysis, we did not observe a significant difference in the rate of respiratory complications between the transhiatal and transthoracic approaches.
Conclusion: Esophageal cancer is a malignant disease whose curative treatment is surgical esophagectomy. Esophagectomy should unequivocally be performed in specialized centers experienced in the treatment of this serious malignancy (High volume centers) and by knowledgeable oncosurgeons with many years of experience with esophageal surgery.