
Keywords
lymph nodes
H&E
IHC CK19
OSNA assay
Abstract
Introduction: The aim of this article is to compare the sensitivity of detecting micrometastases in hilar and mediastinal lymph nodes in case of primary (non-small cell) and secondary (metastases of colorectal carcinoma) pulmonary tumours using standard histopathological examination with haematoxylin-eosin staining, immunohistochemistry examination with Anti-Cytokeratin 19 antibody and examination based on the One-Step Nucleic Acid Amplification method.
Method: During radical surgical treatment of primary non-small cell lung carcinoma and pulmonary metastases of colorectal carcinoma, hilar and mediastinal lymph nodes of 100 patients enrolled in the study in the period from 2015 to 2017 were extracted based on a standard classification. These lymph nodes were subsequently divided along the longitudinal axis into 4 identical parts where part one and three on the left were intended for examination based on the One-Step Nucleic Acid Amplification method, whereas parts two and four were subjected to histopathological examination. In evaluating the respective parts of the nodes by histological examination, the nodes were first examined by a standard procedure that involves haematoxylin-eosin staining, followed by immunohistochemistry examination with Anti-Cytokeratin 19 antibody. The One-Step Nucleic Acid Amplification method was performed in the kit supplied by Sysmex (Kobe, Japan) and is based on the detection of cytokeratin 19 mRNA (messenger ribonucleic acid) by reverse transcription coupled with isothermal amplification.
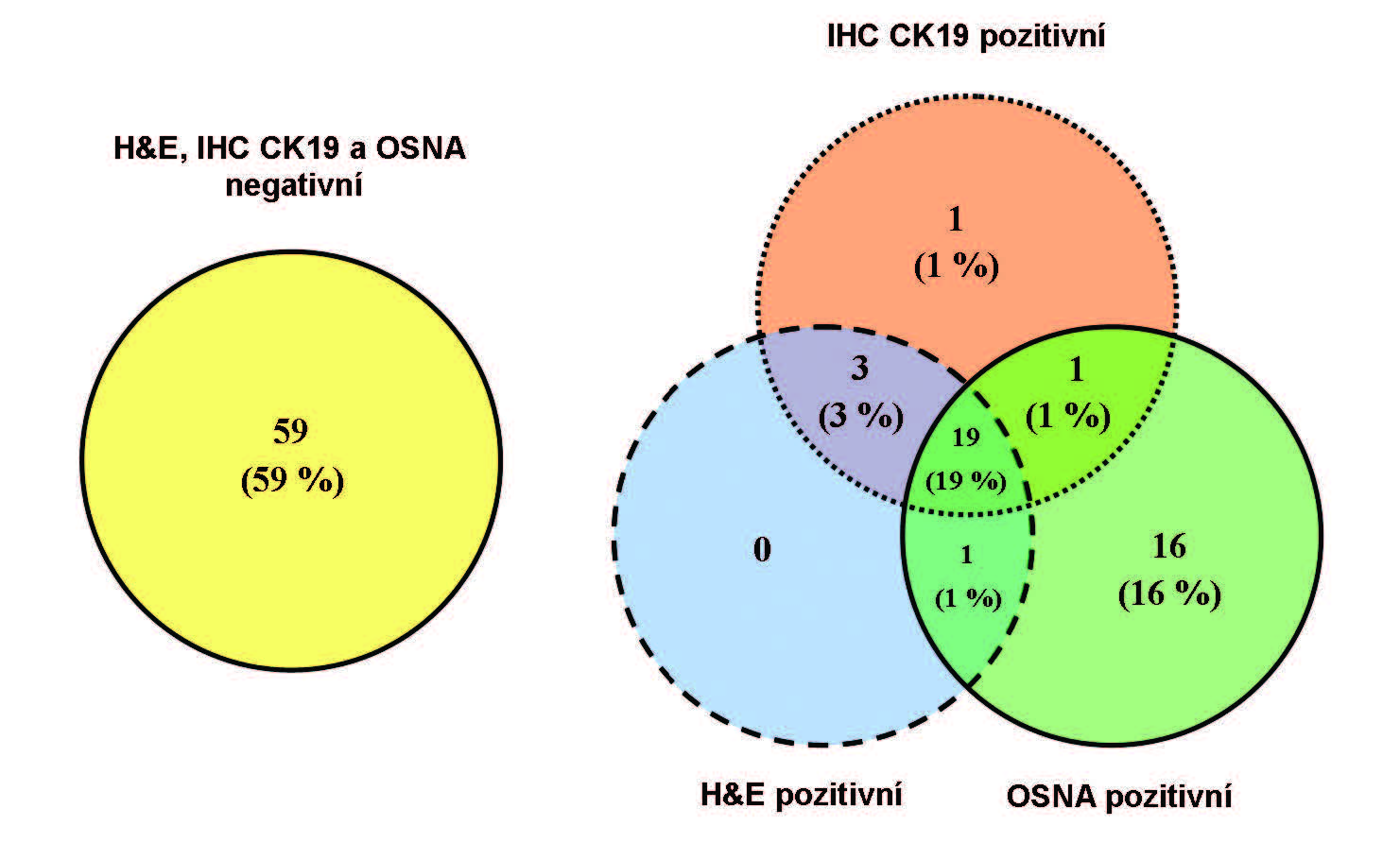
Results: A total of 1,426 lymph nodes of the patients enrolled in the study were extracted and examined using the above mentioned methodology. In 78 patients (78%), identical results were obtained using haematoxylin-eosin staining, immunohistochemistry with Anti-Cytokeratin 19 and One- Step Nucleic Acid Amplification. Micrometastases in the lymph nodes using the One-Step Nucleic Acid Amplification method in the absence of the other methods were proven in 16 patients (16%). Only in 3 cases (3%), the examination by haematoxylin-eosin staining, or immunohistochemistry with Anti-Cytokeratin 19, was positive while One-Step Nucleic Acid Amplification was negative. The results obtained by immunohistochemistry with Anti-Cytokeratin 19 antibody were practically the same as those obtained by haematoxylin-eosin staining (97%).
Conclusion: The results of the study have demonstrated a higher percentage of metastases detected in hilar and mediastinal lymph nodes if the One-Step Nucleic Acid Amplification method of examination was used compared to haematoxylin-eosin staining and immunohistochemistry with Anti-Cytokeratin 19 antibody (upstaging in 16%). This shows that the examination of lymph nodes using the One-Step Nucleic Acid Amplification method can have a certain potential to make the pulmonary tumours staging more accurate. On the other hand, immunohistochemistry with Anti- Cytokeratin 19 antibody seems to be not so useful. However, it is necessary to prove this hypothesis in follow-up studies, or where applicable, in a larger cohort of patients. Another task is to ascertain, by careful patient monitoring, the influence of the micrometastases detected in their lymph nodes using the One-Step Nucleic Acid Amplification method on these patients’ follow-up.