
Keywords
Abstract
Introduction: Histological examination during surgery (FS) has a place in the surgical management of differentiated thyroid carcinoma (DTC). Extending the indication for limited surgery to 4 cm tumor size (ATA guidelines 2015) cytologically verified DTCs, increases the emphasis on accurate patient selection. In our work, we reflected on the effectiveness of FS and its relationship to optimal patient management.
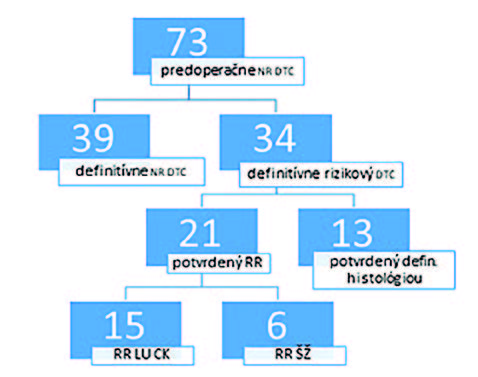
Methods: In a single-center retrospective study, we evaluated the documentation of patients indicated for primary surgery for DTC from January 1, 2016 to December 31, 2020 – there was 489 patients collectively, 121 were men, median age was 50 years (16−81), 73 patients (female, age 18−45 years) with preoperatively identified low-risk DTC (size 11−40mm) were indicated for lobectomy.
Results: 34 patients (46.6%) did not meet the criteria for limited surgery − 15 patients were identified from FS of the lymph nodes of the central compartment (LNCK) (15 of 25 patients) – 1 patient with false negative result and 6 patients with FS of the thyroid gland (SH) (6 / 41) – 11 patients with false negative findings. Two-step OP surgery was performed on 13 patients (17.8%). FS of LNCK identified high-risk cancer and reduced the risk of two-step surgery compared to the group of patients in whom FS was not performed or was performed from thyroid gland. The difference was statistically significant (OR 1.93, p=0.026).
Conclusion: Approximately ½ of the patients from preoperatively identified low-risk cancers in our cohort met the criteria for limited surgery. About 30% of them eventually needed a two-step operation. Perioperative examination of LNCK helps to perform radical surgery at one time