
Keywords
esophageal leakage
esophagectomy complications
intraoperative endoscopy
Abstract
Introduction: Post-oesophagectomy leakage occurs in 1−30% of cases as a significant factor in postoperative morbidity and mortality, accounting for 40% of postoperative deaths. Endoscopic vacuum therapy (EVAC) is, besides stent therapy, clips and surgical therapy, a new endoscopic therapeutic modality.
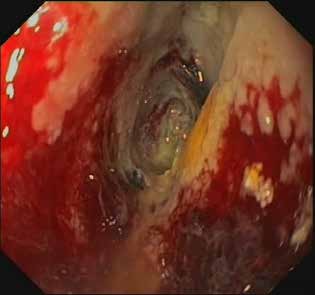
Case report: A 72-year-old polymorbid female patient with Siewert type II adenocarcinoma of the distal esophagus (T1b, N0, M0) was indicated for resection of the upper stomach and lower thoracic esophagus from laparotomy and thoracotomy with reconstruction using double-stapling anastomosis. On postoperative day 12, a 3rd degree leakage with propagation into the right pleural cavity was proven on CT. Endoscopy showed a defect affecting 30% of the circumference with a 7×3×3 cm cavity. Because of the leak morphology, EVAC was indicated. The therapy comprised 12 sessions with 3−4-day intervals for a total duration of 40 days with 5 extraluminal and 7 intraluminal applications and negative pressure of 100−125 mmHg. The condition was complicated by global respiratory failure due to severe pneumonia. Artificial ventilation was terminated on the 58th postoperative day. The patient was discharged to a rehabilitation facility on the 90th postoperative day. The follow-up 3 months after discharge confirms satisfactory performance results with full replenishment.
Conclusion: The therapy of complications of intrathoracic anastomoses after oesophagectomy has shown a trend toward reduced invasiveness and wider implementation of endoscopic methods. In spite of its shortcomings, the use of EVAC is a safe and highly effective therapeutic option even for extensive anastomotic defects. The future use, indications as well as relation to other therapeutic options require further evaluation.