
Abstract
Introduction: The ureter is present in surgical field during inguinal hernia repair in 0.5–4% of cases. It typically occurs in obese patients, in men and patients after kidney transplants. Right-sided and indirect location of ureteral herniation prevails. The clinical picture is mostly asymptomatic, but possible manifestations include increased frequency of urination with urgency, nocturia, recurrent pyelonephritis, urosepsis, feeling of incomplete emptying of the bladder, signs of GIT obstruction. Diagnostic methods include retrograde pyelography or CT urography. Surgical treatment is indicated in every case of ureteral herniation. Reposition of the ureter retroperitoneally and standard plasty of the inguinal canal is the method of choice.
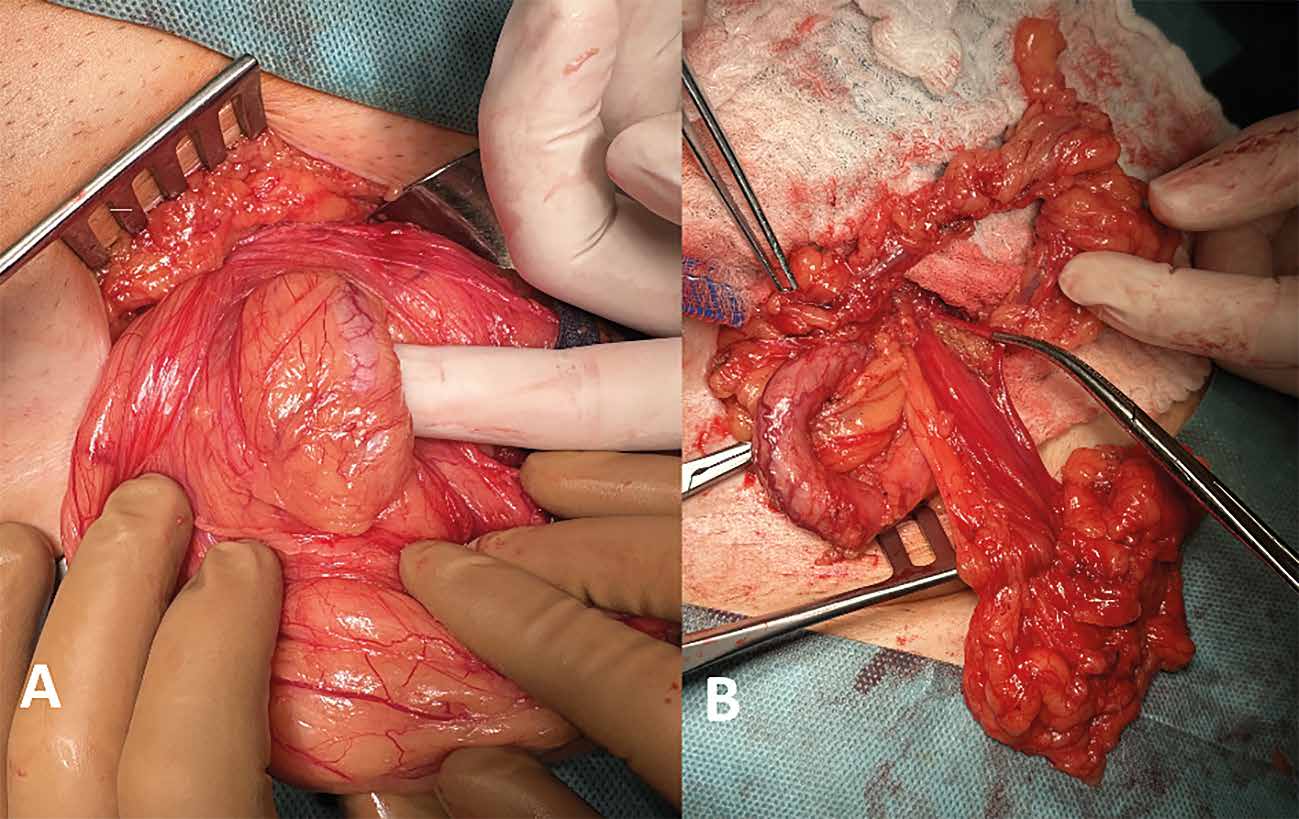
Methods: 33 cases of ureteral hernia were reviewed in order to write a systematized review of the topic. The case report describes a 68-year-old patient with prostatic hyperplasia and dysuria treated at our institution. A preoperative CT examination with intravenous contrast showed herniation of the right ureter into the inguinal area with hydronephrosis of 2nd degree. Preoperative insertion of a mono-J stent into the right ureter and reposition of the ureter retroperitoneally followed by hernia repair using alloplastic material was performed. There were no postoperative complications.
Results and conclusion: In risky cases, the surgeon should assume the possible presence of a ureter in the inguinal region. Careful dissection in the inguinal area reduces the risk of iatrogenic damage to the ureter.